Distinguishing between blisters and warts represents one of the most common diagnostic challenges in dermatological practice. These two distinct skin conditions frequently cause confusion among patients and healthcare providers alike, primarily due to their occasional similarity in appearance during certain stages of development. Understanding the fundamental differences between these lesions is crucial for appropriate treatment decisions and preventing unnecessary complications.
While both conditions affect the skin’s surface, they arise from entirely different pathophysiological mechanisms. Blisters result from fluid accumulation within or beneath the epidermis, typically following trauma, thermal injury, or inflammatory processes. Conversely, warts develop as benign epithelial proliferations caused by human papillomavirus infection, creating characteristic hyperkeratotic lesions with distinctive morphological features.
The clinical significance of accurate differentiation extends beyond mere academic interest. Misidentification can lead to inappropriate treatment protocols , delayed healing, or unnecessary patient anxiety. Moreover, understanding these differences enables healthcare professionals to provide targeted therapeutic interventions and appropriate patient education regarding transmission risks and prognosis.
Clinical identification of cutaneous blisters: vesicle and bullae characteristics
Cutaneous blisters manifest as fluid-filled elevations of the skin, presenting in two primary morphological variants based on their diameter. Vesicles, measuring less than one centimetre, and bullae, exceeding one centimetre in diameter, share fundamental structural characteristics despite their size differences. These lesions develop when serous fluid accumulates either within the epidermis (intraepidermal) or at the dermoepidermal junction (subepidermal), creating the characteristic dome-shaped elevation that defines blister morphology.
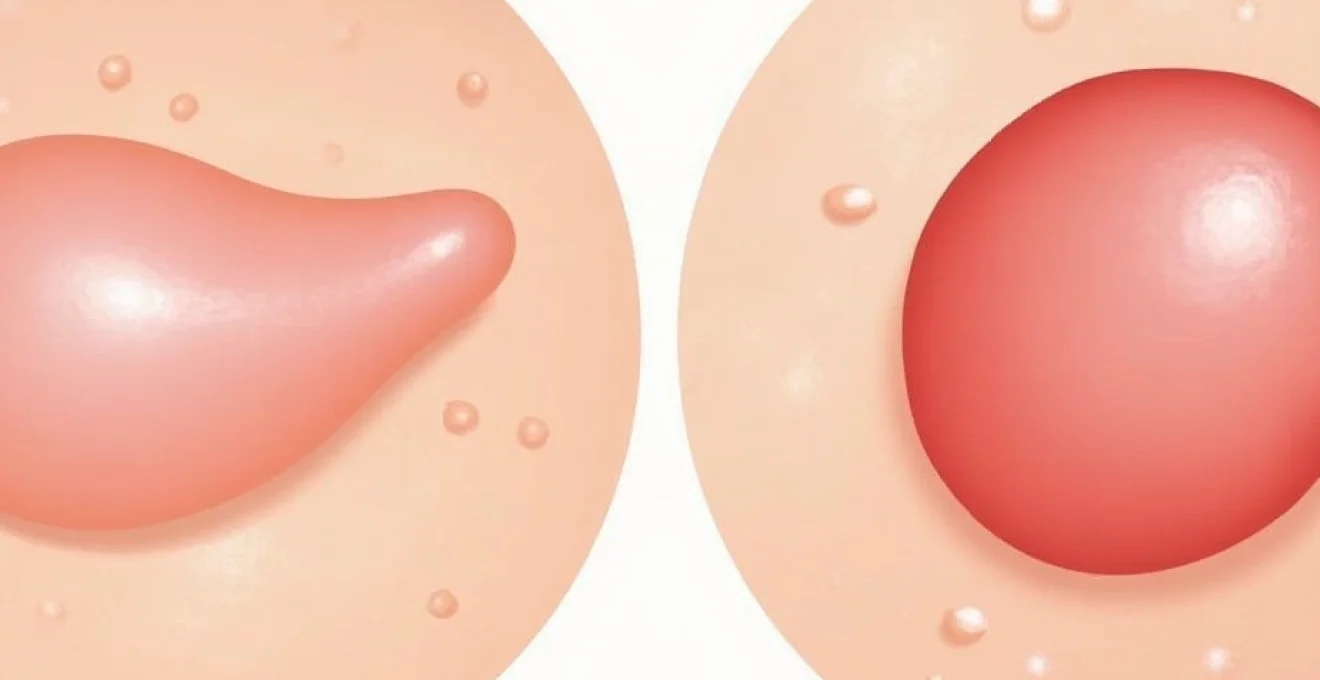
The clinical presentation of blisters varies significantly depending on their underlying aetiology and anatomical location. Fresh blisters typically appear as tense, translucent elevations with smooth, glistening surfaces that reflect light uniformly. The contained fluid may range from clear serous exudate to haemorrhagic content, depending on the degree of capillary involvement and the underlying pathological process.
Fluid-filled vesicle formation and serous exudate properties
The formation of vesicles involves complex pathophysiological mechanisms that result in fluid accumulation within tissue planes. Serous exudate, the primary constituent of blister fluid, contains proteins, electrolytes, and cellular debris derived from the surrounding tissue. This fluid typically maintains a clear to slightly amber appearance, though inflammatory processes may introduce additional cellular components that alter its characteristics.
The protein composition of blister fluid provides valuable diagnostic information, as different aetiologies produce distinct biochemical profiles. Friction-induced blisters typically contain lower protein concentrations compared to those resulting from inflammatory or autoimmune processes. This difference reflects the varying degrees of vascular permeability and tissue disruption associated with different causative mechanisms.
Friction-induced blister development on palmar and plantar surfaces
Mechanical friction represents the most common cause of blister formation, particularly affecting areas subjected to repetitive trauma or prolonged pressure. The palmar and plantar surfaces, with their thick stratum corneum and high mechanical stress exposure, demonstrate increased susceptibility to friction-induced vesiculation. These blisters typically develop following activities involving repetitive motion, such as prolonged walking, manual labour, or sports participation.
The pathophysiology of friction blisters involves shear forces that cause separation between tissue layers, creating potential spaces for fluid accumulation. Initial tissue damage triggers an inflammatory response, resulting in increased vascular permeability and subsequent serous fluid extravasation. The anatomical characteristics of palmar and plantar skin, including increased epidermal thickness and enhanced adherence to underlying structures, influence both the likelihood of blister formation and their clinical presentation.
Thermal burn blister pathophysiology and epidermis separation
Thermal injury represents a significant cause of blister formation, with the severity and depth of tissue damage determining the resulting clinical manifestation. Second-degree burns characteristically produce blisters as the thermal energy disrupts cellular integrity and vascular structures within the dermis. The resulting inflammatory response leads to increased capillary permeability and fluid extravasation into the tissue spaces.
The mechanism of epidermis separation in thermal injuries involves protein denaturation and cellular necrosis that weakens the structural bonds between tissue layers. Temperature exposure duration and intensity directly correlate with the extent of tissue separation and subsequent blister formation. Understanding these relationships helps clinicians assess injury severity and develop appropriate treatment protocols for thermal burn patients.
Contact dermatitis bullous reactions and allergenic triggers
Allergic and irritant contact dermatitis can produce bullous reactions through immune-mediated and direct cytotoxic mechanisms respectively. Common allergenic triggers include plant toxins, metals, preservatives, and industrial chemicals that initiate type IV hypersensitivity reactions. These immunological processes result in inflammatory mediator release and subsequent tissue oedema that manifests as blister formation.
The temporal relationship between exposure and blister development varies significantly based on the underlying mechanism. Irritant reactions may develop within hours of contact, whilst allergic responses typically require 24-48 hours for full manifestation. This timing difference provides valuable diagnostic information when evaluating patients with suspected contact dermatitis and associated bullous lesions.
Viral wart morphology: HPV-Induced epidermal hyperplasia patterns
Human papillomavirus infection produces characteristic morphological changes in infected epidermal tissue, resulting in the distinctive appearance of viral warts. The viral cytopathic effects stimulate abnormal keratinocyte proliferation and differentiation, creating hyperkeratotic lesions with specific architectural patterns. These changes reflect the virus’s ability to manipulate cellular growth mechanisms and interfere with normal epidermal maturation processes.
The morphological diversity of viral warts correlates with different HPV subtypes and their tissue tropism. Each viral strain demonstrates preferential infection patterns for specific anatomical sites and produces characteristic histological changes. Understanding these relationships enables clinicians to identify likely viral aetiologies based on lesion morphology and anatomical distribution patterns.
The viral manipulation of keratinocyte growth cycles creates distinctive hyperplastic patterns that serve as diagnostic hallmarks for different wart subtypes.
Common wart hyperkeratosis and papillomatous surface texture
Common warts, typically caused by HPV types 1, 2, and 4, demonstrate characteristic hyperkeratotic surfaces with papillomatous texture that distinguishes them from other skin lesions. The viral infection disrupts normal keratinocyte maturation, resulting in excessive keratin production and abnormal surface architecture. These changes create the distinctive “cauliflower-like” appearance that defines common wart morphology.
The hyperkeratotic surface of common warts serves multiple viral functions, including protection from environmental factors and facilitation of viral transmission through desquamated infected cells. The degree of hyperkeratosis often correlates with lesion age and viral load , with older, more established infections typically demonstrating more pronounced surface changes. This relationship provides valuable information regarding lesion chronicity and potential treatment responsiveness.
Plantar wart callus formation and Weight-Bearing pressure points
Plantar warts develop unique morphological characteristics due to the mechanical pressures associated with weight-bearing activities. Unlike warts in other anatomical locations, plantar lesions grow inward rather than outward, creating painful pressure points that significantly impact patient mobility. The surrounding callus formation represents a reactive response to chronic pressure and friction associated with the underlying viral lesion.
The clinical presentation of plantar warts includes characteristic features that aid in differential diagnosis. Black dots or petechiae within the lesion represent thrombosed capillary loops, a pathognomonic sign that helps distinguish plantar warts from simple calluses or corns. The interruption of dermatoglyphic patterns and the presence of pain upon lateral compression further support the diagnosis of viral aetiology.
Flat wart minimal elevation and facial distribution patterns
Flat warts, primarily caused by HPV types 3 and 10, demonstrate minimal surface elevation and smooth textures that can complicate clinical recognition. These lesions typically appear as slightly raised, flesh-coloured or light brown papules with diameters ranging from 1-4 millimetres. Their subtle appearance often leads to delayed recognition and inadvertent spread through activities such as shaving or facial cleansing.
The facial distribution pattern of flat warts reflects both viral tropism and transmission mechanisms. These lesions commonly occur in linear arrays following trauma patterns, such as shaving tracks or scratching lines. The tendency for flat warts to appear in clusters or linear configurations provides valuable diagnostic information and helps differentiate them from other facial skin conditions such as seborrhoeic keratoses or solar lentigines.
Filiform wart elongated projections and perioral localisation
Filiform warts present as elongated, finger-like projections that extend from narrow stalks attached to the skin surface. These distinctive lesions typically develop in areas of frequent mechanical irritation, particularly around the mouth, nose, and eyelids. The unique morphology reflects specific viral-host interactions that favour vertical growth patterns over horizontal expansion.
The perioral localisation of filiform warts creates both aesthetic and functional concerns for affected patients. The prominent projections may interfere with normal activities such as eating, speaking, or facial expressions. Additionally, the fragile nature of these lesions makes them susceptible to trauma and secondary bacterial infection, particularly in areas subjected to frequent contact or manipulation.
Histopathological differences: intraepidermal fluid accumulation vs viral cytopathic effects
Microscopic examination reveals fundamental structural differences between blisters and warts that reflect their distinct pathogenic mechanisms. Blisters demonstrate characteristic fluid-filled cavities within or beneath the epidermis, with surrounding tissue showing varying degrees of inflammatory infiltration depending on the underlying aetiology. The cavity formation results from cell separation or destruction, creating spaces for serous fluid accumulation.
In contrast, viral warts exhibit characteristic cytopathic changes including koilocytosis, hyperkeratosis, and acanthosis that reflect HPV infection effects on keratinocyte biology. These changes include nuclear enlargement, cytoplasmic vacuolisation, and altered cellular differentiation patterns that create the distinctive histological appearance of viral lesions. The presence of viral inclusions and specific protein markers further confirms the viral aetiology.
The inflammatory patterns associated with these conditions also demonstrate significant differences. Blister formation typically involves acute inflammatory responses with neutrophil infiltration and vascular changes, whilst viral warts show chronic inflammatory patterns with lymphocytic infiltration and altered immune responses. These histological differences provide definitive diagnostic information when clinical features alone prove insufficient for accurate differentiation.
Immunohistochemical techniques can further enhance diagnostic accuracy by identifying specific viral proteins or cellular markers associated with different conditions. HPV detection methods, including in situ hybridisation and PCR-based techniques, provide definitive confirmation of viral aetiology in suspected wart lesions. Similarly, specific inflammatory markers can help characterise the underlying mechanisms responsible for blister formation in complex cases.
Diagnostic dermoscopy techniques for lesion differentiation
Dermoscopic examination provides valuable diagnostic information for differentiating between blisters and warts through enhanced visualisation of surface morphology and internal structures. This non-invasive technique reveals microscopic details invisible to naked-eye examination, enabling more accurate diagnosis and reducing the need for invasive procedures. The specific dermoscopic patterns associated with different lesion types serve as reliable diagnostic markers in clinical practice.
The application of dermoscopy requires systematic evaluation of lesion characteristics including surface texture, colour patterns, vascular structures, and architectural features. Different magnification levels and polarisation settings reveal distinct features that aid in diagnostic differentiation. Standardised dermoscopic terminology ensures consistent interpretation and facilitates communication between healthcare providers regarding specific findings.
Capillary loop patterns in wart papillary dermis visualisation
Dermoscopic examination of viral warts reveals characteristic capillary loop patterns within the papillary dermis that serve as diagnostic hallmarks. These vascular structures appear as red dots or hairpin-shaped vessels surrounded by whitish halos, reflecting the underlying papillomatous architecture of viral lesions. The regular distribution and specific morphology of these capillary loops help distinguish warts from other hyperkeratotic conditions.
The capillary loop patterns demonstrate variations depending on wart type and anatomical location. Common warts typically show prominent, regularly distributed capillary loops, whilst flat warts may exhibit more subtle vascular patterns. The identification of these specific vascular signatures provides valuable diagnostic information and helps guide appropriate treatment selection based on lesion characteristics.
Black dot appearance in thrombosed capillaries of plantar warts
Plantar warts demonstrate characteristic black dot appearances under dermoscopic examination, representing thrombosed capillary loops within the lesion architecture. These dark spots result from blood coagulation within dilated capillary vessels subjected to repeated mechanical trauma from weight-bearing activities. The presence and distribution of these black dots serve as pathognomonic signs that distinguish plantar warts from calluses or other hyperkeratotic foot lesions.
The number and size of black dots often correlate with lesion maturity and viral activity levels. Fresh or actively growing plantar warts typically demonstrate numerous prominent black dots, whilst older or resolving lesions may show fewer or smaller vascular changes. This relationship provides prognostic information regarding treatment responsiveness and expected healing timelines.
Smooth blister surface reflectance under dermatoscopic examination
Dermoscopic examination of blisters reveals characteristic smooth surface reflectance patterns that reflect their fluid-filled nature and intact overlying epidermis. The uniform light reflection from the blister surface creates distinctive optical properties that differ markedly from the irregular surface textures observed in viral warts. These optical characteristics provide reliable diagnostic information for lesion differentiation.
The fluid content and internal structure of blisters create specific dermoscopic patterns that vary depending on the underlying aetiology and lesion age. Fresh blisters typically demonstrate uniform internal appearances with clear fluid content, whilst older lesions may show fibrin deposits, cellular debris, or haemorrhagic changes that alter their dermoscopic characteristics.
Treatment protocols: cryotherapy for warts vs conservative blister management
Treatment approaches for blisters and warts differ fundamentally based on their distinct pathophysiological mechanisms and natural histories. Viral warts require active intervention to eliminate infected tissue and prevent viral transmission, whilst blister management focuses on preventing secondary complications and promoting natural healing processes. Understanding these different therapeutic philosophies ensures appropriate treatment selection and optimal patient outcomes.
Cryotherapy represents the gold standard treatment for most viral warts, utilising controlled tissue destruction through freeze-thaw cycles that eliminate infected keratinocytes. The technique involves applying liquid nitrogen or other cryogenic agents to achieve temperatures of -50 to -60 degrees Celsius, sufficient to destroy viral-infected cells whilst preserving underlying healthy tissue. Multiple treatment sessions are typically required to achieve complete viral eradication and prevent recurrence.
Conservative blister management emphasises protection of the natural barrier function whilst preventing secondary bacterial infection. Intact blisters should generally remain undisturbed, as the overlying epidermis provides optimal protection against contamination. When drainage becomes necessary due to size or discomfort, sterile technique and appropriate wound care protocols minimise complications and promote healing.
The fundamental difference in treatment philosophy reflects the self-limiting nature of blisters versus the persistent, transmissible character of viral warts.
Treatment success rates vary significantly between these conditions, with viral warts demonstrating higher recurrence rates and variable treatment responsiveness compared to blisters. Factors influencing treatment outcomes include patient immune status, lesion characteristics, anatomical location, and compliance with therapeutic protocols. Understanding these variables helps clinicians develop realistic treatment expectations and appropriate follow-up schedules.
Alternative treatment modalities for warts include topical chemotherapy agents, immunomodulators, and surgical excision techniques, each with specific indications and contraindications. Blister treatment alternatives focus on protective dressings, pain management, and infection prevention strategies. The selection of specific treatment approaches requires consideration of patient factors, lesion characteristics, and individual risk-benefit profiles.
Differential diagnosis pitfalls: molluscum contagiosum and dyshidrotic eczema considerations
Several conditions can mimic the appearance of blisters or warts, creating diagnostic challenges that require careful clinical evaluation and sometimes additional testing for accurate differentiation. Molluscum contag
iosum represents a common viral skin condition that can be confused with both blisters and warts, particularly in paediatric populations. These dome-shaped lesions with central umbilication may initially resemble small blisters, especially when the characteristic central depression is not yet fully developed. However, molluscum lesions maintain their solid nature and demonstrate the pathognomonic pearly appearance with central keratotic plug that distinguishes them from fluid-filled vesicles.The viral aetiology of molluscum contagiosum shares similarities with warts, as both conditions result from viral infections affecting epidermal keratinocytes. However, molluscum is caused by a poxvirus rather than HPV, resulting in different clinical presentations and treatment responses. The self-limiting nature of molluscum lesions contrasts with the persistent character of most viral warts, requiring different therapeutic approaches and patient counselling regarding expected outcomes.Dyshidrotic eczema presents another diagnostic challenge, particularly when evaluating vesicular eruptions on the hands and feet. This condition produces characteristic clusters of deep-seated vesicles along the lateral aspects of fingers and palms, which can be mistaken for friction blisters or early wart development. The intense pruritus and recurring nature of dyshidrotic eczema help distinguish it from simple mechanical blisters, whilst the vesicular rather than hyperkeratotic presentation differentiates it from viral warts.The inflammatory nature of dyshidrotic eczema creates additional diagnostic complexity, as secondary changes from scratching and manipulation can obscure the underlying vesicular pattern. Chronic cases may develop lichenification and hyperkeratotic changes that further complicate differentiation from viral lesions. Understanding these evolutionary patterns helps clinicians recognize dyshidrotic eczema at different stages and avoid misdiagnosis.Additional conditions requiring consideration include seborrhoeic keratoses, which may occasionally present with surface changes resembling viral warts, and bullous pemphigoid, which produces large blisters that can be confused with thermal injury or severe contact dermatitis. The age demographics, anatomical distribution patterns, and associated symptoms provide valuable clues for distinguishing these conditions from the primary differential considerations of blisters versus warts.Diagnostic uncertainty often arises when lesions demonstrate atypical presentations or occur in unusual anatomical locations. In such cases, additional diagnostic modalities including dermoscopy, histopathological examination, or viral detection techniques may be necessary for definitive diagnosis. The clinical cost of misdiagnosis includes inappropriate treatment selection, delayed healing, and potential complications that underscore the importance of accurate initial evaluation.The temporal evolution of these various conditions provides additional diagnostic information that clinicians can utilise for differentiation purposes. Blisters typically demonstrate rapid onset and resolution patterns, whilst viral warts show gradual development and persistence without intervention. Molluscum lesions follow intermediate timelines with eventual spontaneous resolution, and dyshidrotic eczema demonstrates cyclical patterns with acute exacerbations and remissions. Understanding these natural histories enables more accurate diagnostic assessment and appropriate patient counselling regarding expected outcomes.Environmental and occupational factors also influence the differential diagnosis process, as certain exposures predispose individuals to specific types of skin lesions. Healthcare workers, food handlers, and individuals with frequent water exposure demonstrate increased risks for certain types of contact dermatitis and associated bullous reactions. Similarly, immunocompromised patients show altered presentations and increased susceptibility to viral infections that may complicate standard diagnostic approaches.The psychological impact of misdiagnosis extends beyond physical consequences, as patients may experience anxiety regarding transmissibility, scarring potential, or treatment duration based on incorrect initial assessments. Providing accurate diagnostic information and realistic treatment expectations helps maintain patient confidence and compliance with recommended therapeutic interventions. This aspect of care proves particularly important for visible lesions that affect patient self-image and social interactions.