Post-nasal drip affects millions of people worldwide, causing uncomfortable symptoms that can significantly impact daily life. When excessive mucus accumulates and drains down the back of your throat, it often triggers an involuntary gagging response that can be both distressing and socially embarrassing. This physiological reaction occurs when the throat’s sensitive tissues become irritated by the constant presence of thick or excessive secretions, leading to pharyngeal hyperresponsiveness and chronic discomfort.
Understanding the complex mechanisms behind post-nasal drip and its associated gagging reflex is crucial for developing effective treatment strategies. The condition affects approximately 20% of the adult population, with symptoms ranging from mild throat clearing to severe retching episodes that interfere with sleep and professional activities. Modern medical research has identified numerous contributing factors, from allergic responses to structural abnormalities, each requiring tailored therapeutic approaches to achieve optimal symptom relief.
Understanding Post-Nasal drip physiology and gagging response mechanisms
The human respiratory system produces between one to two litres of mucus daily, a vital secretion that serves multiple protective functions within the upper airways. This complex process involves specialised goblet cells and submucosal glands distributed throughout the nasal cavity, paranasal sinuses, and throat tissues. Under normal circumstances, this mucus production maintains optimal humidity levels, traps airborne particles, and provides antimicrobial protection against pathogens attempting to penetrate the respiratory tract.
Mucus production pathways in nasal cavity and paranasal sinuses
The nasal cavity’s intricate structure includes turbinates, which create turbulent airflow patterns that enhance the warming and humidification process. Within this environment, ciliated epithelial cells work continuously to transport mucus towards the throat through coordinated wave-like movements. When this delicate system becomes disrupted by inflammation, infection, or structural abnormalities, mucus consistency changes dramatically, becoming thicker and more viscous than normal.
Paranasal sinuses contribute significantly to overall mucus production, with the maxillary, frontal, ethmoid, and sphenoid sinuses each producing specific quantities of secretions. These hollow spaces within the skull bones are lined with mucous membranes that respond dynamically to environmental changes, hormonal fluctuations, and immune system activation. When sinus drainage becomes impaired, accumulated secretions create ideal conditions for bacterial colonisation and chronic inflammation.
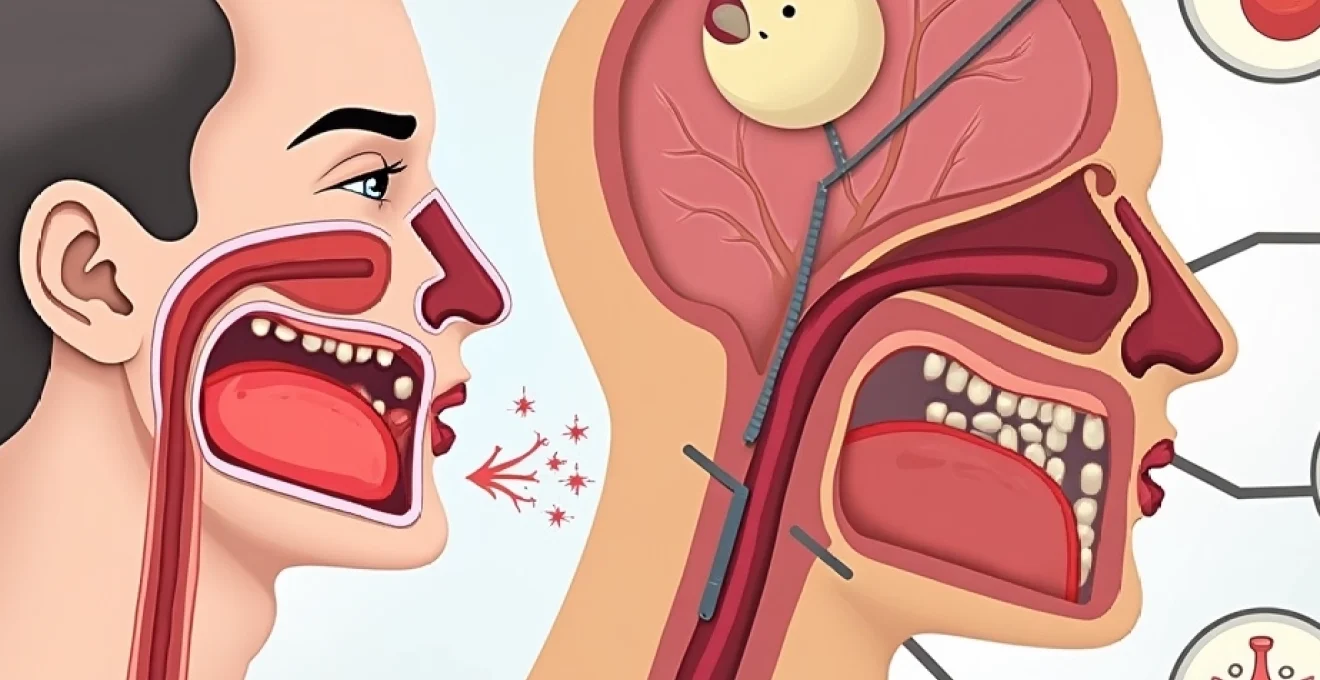
Vagus nerve stimulation and pharyngeal reflex activation
The gagging response associated with post-nasal drip involves complex neurological pathways centered around the vagus nerve, which innervates much of the upper digestive and respiratory tract. When excessive or particularly thick mucus contacts sensitive pharyngeal tissues, mechanoreceptors and chemoreceptors trigger immediate protective reflexes designed to prevent aspiration into the lower airways. This evolutionary mechanism, whilst protective, becomes problematic when continuously activated by chronic drainage.
Pharyngeal hyperresponsiveness develops when these neural pathways become sensitised through repeated stimulation. Research indicates that individuals with chronic post-nasal drip demonstrate significantly lower thresholds for gag reflex activation compared to healthy controls, suggesting that prolonged exposure to irritating secretions creates lasting changes in nerve sensitivity patterns.
Upper respiratory tract anatomy affecting mucus drainage
The anatomy of your upper respiratory tract plays a crucial role in determining drainage patterns and susceptibility to post-nasal drip symptoms. The nasopharynx, located behind the nasal cavity, serves as a critical junction where secretions from various sources converge before proceeding down the throat. Variations in this anatomical structure, including adenoid hypertrophy or nasopharyngeal narrowing, can significantly impact drainage efficiency.
Eustachian tube dysfunction often accompanies post-nasal drip, creating additional complications as mucus blocks these narrow passages connecting the middle ear to the throat. This blockage can lead to ear pressure, hearing difficulties, and secondary infections that further exacerbate mucus production. The relationship between these anatomical structures demonstrates why comprehensive treatment approaches must address multiple interconnected systems rather than focusing solely on mucus reduction.
Histamine response and inflammatory cascade triggering excess secretions
Allergic responses represent one of the most significant contributors to post-nasal drip through histamine-mediated inflammatory cascades. When allergens contact nasal tissues, mast cells release histamine and other inflammatory mediators that dramatically increase vascular permeability and stimulate mucus gland activity. This process can increase normal mucus production by 300-500%, overwhelming the natural drainage mechanisms and creating the characteristic thick, persistent secretions.
The inflammatory response extends beyond simple histamine release, involving complex interactions between leukotrienes, prostaglandins, and cytokines that perpetuate tissue swelling and hypersecretion. Understanding these pathways has led to targeted therapeutic approaches using antihistamines, leukotriene inhibitors, and anti-inflammatory medications that address root causes rather than merely managing symptoms.
Clinical identification of Post-Nasal drip induced gagging symptoms
Accurate diagnosis of post-nasal drip-induced gagging requires careful evaluation of symptom patterns, timing, and associated manifestations. Healthcare professionals typically employ comprehensive assessment techniques including detailed patient histories, physical examinations, and specialized diagnostic procedures to differentiate this condition from other causes of chronic throat irritation. The diagnostic process must consider the wide spectrum of presentations, as symptoms can vary significantly between individuals and may fluctuate based on environmental factors, seasonal changes, and underlying health conditions.
Chronic cough with throat clearing behaviours
The persistent cough associated with post-nasal drip often follows distinctive patterns that help clinicians identify the underlying cause. Unlike coughs related to lower respiratory tract infections, post-nasal drip coughs typically worsen during nighttime hours when lying flat allows accumulated secretions to pool in the throat. Patients frequently describe a tickling sensation that triggers irrepressible urges to cough or clear their throat, creating cycles of irritation and inflammation.
Throat clearing behaviours become habitual responses to the constant sensation of mucus accumulation, but paradoxically, these actions often worsen the underlying irritation. The forceful airflow generated during throat clearing can damage delicate vocal cord tissues and perpetuate inflammatory responses, creating self-reinforcing cycles of symptom progression. Recognition of these patterns helps distinguish post-nasal drip from other respiratory conditions with similar presentations.
Globus sensation and pharyngeal hyperresponsiveness
Globus sensation , the feeling of having a lump or foreign object lodged in the throat, affects up to 80% of individuals with chronic post-nasal drip. This phenomenon results from heightened sensitivity of pharyngeal tissues combined with the physical presence of thick secretions coating throat structures. The sensation often intensifies during periods of emotional stress, suggesting complex interactions between psychological factors and physiological responses.
Pharyngeal hyperresponsiveness manifests as exaggerated reactions to normal stimuli, including swallowing, speaking, or exposure to mild irritants like temperature changes or airborne particles. This heightened sensitivity develops gradually through chronic exposure to inflammatory mediators present in post-nasal drainage, leading to lasting changes in nerve function and tissue responsiveness that persist even during periods of reduced mucus production.
Morning gagging episodes and nocturnal mucus accumulation
Morning gagging episodes represent one of the most characteristic features of post-nasal drip, occurring as accumulated secretions from overnight drainage trigger intense pharyngeal reflexes upon awakening. During sleep, the natural swallowing reflex diminishes significantly, allowing mucus to pool in the throat and become increasingly concentrated through water reabsorption processes. This thick, adherent material proves particularly irritating to sensitive throat tissues.
The severity of morning symptoms often correlates directly with sleep position and bedroom environmental factors. Individuals who sleep in completely flat positions typically experience more severe accumulation compared to those who maintain slight head elevation. Dry indoor air, common during heating seasons, exacerbates the problem by increasing mucus viscosity and reducing the effectiveness of natural clearance mechanisms.
Halitosis development from bacterial colonisation
Chronic post-nasal drip creates ideal conditions for bacterial colonisation within throat tissues, leading to characteristic halitosis that differs from typical bad breath. The protein-rich environment provided by accumulated mucus supports growth of anaerobic bacteria that produce sulfur compounds responsible for particularly offensive odours. This bacterial activity also contributes to ongoing tissue irritation and inflammatory responses.
The development of biofilms within thick secretions makes bacterial colonisation particularly resistant to conventional oral hygiene measures. Standard brushing and mouthwash routines prove inadequate for addressing the deeper tissue involvement that characterises post-nasal drip-related halitosis, requiring targeted approaches that address both the underlying drainage issue and secondary bacterial complications.
Medical treatment protocols for severe Post-Nasal drip cases
Severe post-nasal drip cases often require comprehensive medical intervention combining multiple therapeutic modalities to achieve optimal symptom control. Healthcare providers typically initiate treatment with conservative approaches before progressing to more aggressive interventions, carefully monitoring patient response and adjusting protocols based on underlying causative factors. The treatment hierarchy emphasises evidence-based medications that target specific pathophysiological mechanisms whilst minimising adverse effects and drug interactions.
Prescription medications for severe cases frequently include intranasal corticosteroids such as fluticasone propionate or mometasone furoate, which directly address inflammatory processes within nasal and sinus tissues. These medications demonstrate superior efficacy compared to oral alternatives, delivering concentrated anti-inflammatory effects whilst minimising systemic exposure. Clinical studies indicate that consistent use of intranasal steroids reduces mucus production by 40-60% within four to six weeks of initiation.
Anticholinergic agents like ipratropium bromide nasal spray provide targeted intervention for hypersecretion by blocking parasympathetic nerve stimulation of mucus glands. This mechanism proves particularly effective for individuals with predominantly watery secretions rather than thick, inflammatory drainage. The medication works rapidly, often providing noticeable symptom relief within hours of application, making it valuable for acute symptom management during allergen exposure or viral infections.
Systemic approaches may include oral antihistamines, leukotriene receptor antagonists, or short courses of oral corticosteroids for severe inflammatory episodes. Montelukast, a leukotriene receptor antagonist, offers particular benefits for patients with concurrent asthma or aspirin sensitivity, addressing both upper and lower respiratory tract inflammation simultaneously. However, healthcare providers must carefully weigh potential psychiatric side effects against therapeutic benefits when prescribing this medication.
Proton pump inhibitors represent an often-overlooked component of comprehensive treatment protocols, particularly valuable when gastroesophageal reflux contributes to post-nasal drip symptoms. Studies demonstrate that up to 30% of chronic post-nasal drip cases involve laryngopharyngeal reflux as a contributing factor, making acid suppression therapy an essential consideration in treatment-resistant cases.
Recent clinical trials have demonstrated that combination therapy approaches achieve superior outcomes compared to single-agent treatments, with success rates improving from 60% with monotherapy to 85% with appropriately selected combination regimens.
Evidence-based home remedies and Non-Pharmaceutical interventions
Home-based management strategies provide valuable adjunctive support for post-nasal drip treatment, often serving as first-line interventions for mild to moderate symptoms. These approaches focus on optimising natural drainage mechanisms, reducing mucus viscosity, and minimising environmental triggers that exacerbate secretion production. Evidence supporting these interventions comes from numerous clinical studies demonstrating measurable improvements in symptom severity and quality of life measures when consistently applied.
Nasal irrigation techniques using neti pots and saline solutions
Nasal irrigation represents one of the most effective non-pharmaceutical interventions for post-nasal drip management, with clinical studies demonstrating significant symptom reduction in 70-80% of consistent users. The mechanical action of saline irrigation removes accumulated mucus, allergens, and inflammatory mediators whilst providing beneficial moisturisation to dried nasal tissues. Proper technique involves using isotonic or slightly hypertonic saline solutions to avoid tissue irritation or electrolyte imbalances.
The optimal saline concentration for nasal irrigation ranges from 0.9% to 3%, with higher concentrations providing enhanced mucus-thinning effects but potentially causing temporary stinging sensations. Temperature control proves crucial, as solutions between 37-40°C provide maximum comfort and effectiveness. You should always use distilled, sterile, or previously boiled water to eliminate risks of rare but serious infections from waterborne pathogens.
Steam inhalation therapy with eucalyptus and menthol
Steam inhalation therapy provides immediate relief for many individuals suffering from thick, tenacious post-nasal secretions. The warm, humidified air helps restore optimal moisture levels within nasal and throat tissues whilst promoting natural ciliary function that facilitates mucus clearance. Adding essential oils like eucalyptus or menthol enhances therapeutic effects through their natural decongestant and anti-inflammatory properties.
Eucalyptus oil contains compounds such as 1,8-cineole that demonstrate clinically proven mucolytic effects, helping break down thick secretions and reducing viscosity. The optimal concentration for steam inhalation involves adding 2-3 drops of essential oil per litre of hot water, providing therapeutic benefits without causing respiratory irritation. Treatment sessions lasting 10-15 minutes, performed twice daily, typically provide optimal symptom relief without overexposure risks.
Dietary modifications targeting Mucus-Producing foods
Dietary interventions play a significant role in managing post-nasal drip symptoms, particularly for individuals with food sensitivities or inflammatory responses to specific nutritional components. Dairy elimination remains controversial, with some studies suggesting benefits whilst others find no significant correlation between dairy consumption and mucus production. However, individuals who notice symptom improvement with dairy restriction should continue these modifications under appropriate nutritional guidance.
Anti-inflammatory dietary approaches emphasising omega-3 fatty acids, quercetin-rich foods, and natural antihistamine compounds can provide measurable symptom reduction. Foods high in vitamin C, such as citrus fruits (consumed in moderation to avoid acid reflux triggers), support immune function and may reduce inflammatory responses that contribute to excessive secretion production. Spicy foods containing capsaicin can temporarily thin secretions, though they may also trigger increased production in sensitive individuals.
Positional sleep therapy and elevated head rest positioning
Sleep position modifications represent simple yet highly effective interventions for reducing nocturnal mucus accumulation and morning gagging episodes. Elevating the head of your bed by 15-20 degrees promotes gravitational drainage whilst maintaining comfortable sleep positioning. This approach proves more effective than simply using additional pillows, which can create neck strain and potentially worsen symptoms through airway compression.
Side sleeping positions, particularly lying on the side opposite to the most congested nasal passage, can enhance drainage patterns and reduce accumulation in throat tissues. Some individuals benefit from alternating sleep sides throughout the night, though this requires conscious effort that may initially disrupt sleep quality. The use of wedge pillows or adjustable bed frames provides consistent elevation without the positional instability associated with multiple traditional pillows.
Advanced therapeutic approaches and specialist interventions
When conservative treatments fail to provide adequate symptom relief, advanced therapeutic interventions become necessary to address underlying structural abnormalities or persistent inflammatory conditions. These sophisticated approaches require specialist evaluation and often involve surgical or procedural interventions that target specific anatomical or physiological problems contributing to chronic post-nasal drip. The decision to pursue advanced treatments depends on thorough diagnostic evaluation, failed conservative therapy trials, and significant impact on quality of life measures.
Endoscopic sinus surgery for chronic sinusitis management
Functional endoscopic sinus surgery (FESS) represents the gold standard treatment for chronic sinusitis-related post-nasal drip when medical management proves inadequate. This minimally invasive procedure utilises specialised endoscopic techniques to restore normal sinus drainage pathways by removing obstructive tissue, polyps, or structural abnormalities that impede natural clearance mechanisms. Success rates for symptom improvement exceed 85% in appropriately selected candidates, with most patients experiencing significant reductions in post-nasal drip within 6-12 weeks post-operatively.
Modern FESS techniques incorporate computer-guided navigation systems that enhance surgical precision whilst minimising complications and tissue trauma. The procedure focuses on enlarging natural sinus openings rather than creating artificial drainage pathways, preserving normal physiological function whilst improving ventilation and drainage. Post-operative care involves extensive nasal irrigation protocols and close monitoring to prevent adhesion formation and ensure optimal healing outcomes.
Immunotherapy for allergic rhinitis
Allergic rhinitis-related post-nasal drip often requires targeted immunotherapy when conventional antihistamine treatments prove insufficient for long-term symptom control. Subcutaneous immunotherapy (allergy shots) involves gradually increasing doses of specific allergens administered over 3-5 years, with success rates approaching 80-90% for appropriately selected patients. This treatment modality works by inducing immune tolerance through controlled exposure, ultimately reducing the inflammatory cascade that triggers excessive mucus production.
Sublingual immunotherapy offers a convenient alternative to injection-based treatment, utilising allergen extracts placed under the tongue for absorption through oral mucosa. Research demonstrates comparable efficacy to traditional shots with significantly improved safety profiles and patient compliance rates. The treatment requires daily administration for extended periods but eliminates the need for frequent clinic visits and reduces risks of severe allergic reactions associated with injection therapy.
Botulinum toxin injections for hypersalivation control
Botulinum toxin injections represent an innovative approach for managing excessive salivary gland secretions that contribute to post-nasal drip symptoms in selected patients. This treatment targets the parasympathetic nerve endings that stimulate glandular secretion, providing temporary but significant reduction in saliva production that can last 4-6 months per treatment cycle. The procedure involves precise injection techniques guided by ultrasound or electromyography to ensure accurate placement and optimal therapeutic outcomes.
Clinical studies demonstrate symptom improvement in 70-85% of patients with hypersalivation-related post-nasal drip, particularly those with neurological conditions or medication-induced xerostomia. The treatment requires careful patient selection and skilled practitioners familiar with salivary gland anatomy to minimise potential complications such as swallowing difficulties or unwanted muscle weakness. Recovery typically involves mild swelling for 24-48 hours with gradual onset of therapeutic effects over the following week.
Radiofrequency ablation of posterior nasal nerves
Radiofrequency ablation of the posterior nasal nerve (vidian nerve) offers a minimally invasive solution for chronic rhinitis-related post-nasal drip resistant to conventional treatments. This procedure utilises controlled thermal energy to selectively interrupt nerve pathways responsible for excessive glandular secretion whilst preserving normal nasal function. The technique requires endoscopic guidance to ensure precise targeting of nerve structures located deep within the nasal cavity.
Success rates for radiofrequency ablation range from 60-80% for carefully selected candidates, with symptom improvement typically lasting 12-24 months before potential retreatment becomes necessary. The procedure involves local anaesthesia and typically requires 30-45 minutes to complete, with most patients returning to normal activities within 48-72 hours. Post-procedural monitoring includes assessment of nasal function, tear production, and potential complications such as temporary numbness or altered taste sensation.
Long-term management strategies and lifestyle modifications
Successful long-term management of post-nasal drip-related gagging requires comprehensive lifestyle modifications that address environmental triggers, optimise natural drainage mechanisms, and prevent symptom recurrence. The chronic nature of this condition necessitates sustained behavioural changes and ongoing monitoring to maintain optimal quality of life. Research indicates that patients who implement comprehensive lifestyle modification programs achieve 60-70% greater long-term success rates compared to those relying solely on pharmacological interventions.
Environmental control measures form the foundation of effective long-term management, particularly for individuals with allergic sensitivities. Installing high-efficiency particulate air (HEPA) filtration systems reduces airborne allergen exposure by 85-95%, whilst maintaining indoor humidity levels between 40-50% prevents excessive mucus viscosity. Regular replacement of HVAC filters, elimination of dust-collecting furnishings, and strategic use of air purifiers create optimal indoor environments that minimise inflammatory triggers.
Hydration protocols require careful attention to both quantity and timing of fluid intake throughout the day. Consuming 8-10 glasses of water daily helps maintain optimal mucus consistency, but concentrating intake during morning and afternoon hours prevents nocturnal bladder disturbance that can disrupt therapeutic sleep positioning. Warm beverages such as herbal teas provide additional benefits through steam inhalation effects, whilst caffeinated drinks should be limited due to their potential dehydrating properties.
Stress management techniques play an often-underestimated role in post-nasal drip management, as psychological stress can trigger inflammatory responses that exacerbate mucus production. Regular practice of relaxation techniques, including deep breathing exercises, meditation, or yoga, demonstrates measurable benefits in reducing symptom severity and frequency. The mind-body connection becomes particularly important during symptom flares, when anxiety about gagging episodes can create self-perpetuating cycles of increased pharyngeal sensitivity.
Professional monitoring schedules should include regular otolaryngology evaluations every 6-12 months to assess treatment effectiveness and identify emerging complications. These appointments provide opportunities to adjust medication regimens, review home care techniques, and detect early signs of secondary complications such as chronic sinusitis or vocal cord irritation. Documentation of symptom patterns through daily tracking logs helps healthcare providers optimise treatment protocols based on individual response patterns and seasonal variations.
Workplace and social adaptations enable individuals to maintain professional and personal relationships despite chronic symptoms. Discrete management techniques, such as carrying sugar-free lozenges for throat lubrication or scheduling important meetings during optimal symptom control periods, help minimise social embarrassment whilst maintaining productivity. Communication with employers about necessary accommodations, such as access to private spaces for nasal irrigation or modified work schedules during severe symptom periods, ensures continued career success alongside optimal health management.
Long-term studies demonstrate that patients implementing comprehensive lifestyle modification programs alongside appropriate medical treatment achieve sustained symptom improvement in 85% of cases, compared to 45% success rates with medical treatment alone.