Dental trauma can manifest in various ways, but one of the most overlooked forms is tooth bruising, a condition that often goes undetected until significant complications arise. Unlike surface-level dental injuries such as chips or cracks, bruised teeth present subtle visual changes that require trained observation and clinical expertise to identify properly. The appearance of a bruised tooth can vary dramatically depending on the severity of trauma, the time elapsed since injury, and the underlying pathophysiology affecting the pulpal tissues. Understanding these visual indicators is crucial for both dental professionals and patients, as early recognition can mean the difference between successful conservative treatment and eventual tooth loss. The complexity of dental trauma assessment extends beyond simple visual inspection, requiring a comprehensive understanding of how internal tissue damage translates to external manifestations.
Clinical identification of dental trauma through visual assessment
The initial clinical presentation of a bruised tooth often appears deceptively normal to the untrained eye, making visual assessment a critical skill in emergency dental care. Professional evaluation begins with systematic observation under proper lighting conditions, typically using dental operatory lights that provide consistent colour temperature and intensity. The affected tooth may exhibit subtle variations in translucency compared to adjacent healthy teeth, often presenting as a slight dulling of the natural lustre that characterises vital dental tissues.
Periapical discolouration patterns in crown structure
The most distinctive visual indicator of dental trauma involves discolouration patterns that develop within the crown structure, particularly in the cervical and middle thirds of the tooth. These colour changes typically progress through predictable stages, beginning with a subtle pinkish hue that indicates active bleeding within the pulp chamber. The pink discolouration results from haemoglobin infiltration into the dentinal tubules, creating a characteristic appearance that experienced clinicians recognise as an early warning sign of pulpal compromise.
As the condition progresses, the pink coloration may transition to yellow-brown tones, indicating the breakdown of red blood cells and the formation of haemosiderin deposits within the dental tissues. This intermediate stage often presents the greatest diagnostic challenge, as the colour changes may be subtle enough to escape notice during routine visual examination. The final stage typically involves grey to black discolouration, signalling complete pulpal necrosis and the urgent need for endodontic intervention.
Enamel surface irregularities following impact injury
Beyond colour changes, bruised teeth frequently exhibit subtle surface irregularities that become apparent under magnification and proper lighting. These may include microscopic fracture lines running vertically or horizontally across the enamel surface, often invisible to naked-eye examination but clearly visible under dental loupes or microscopic inspection. The enamel may also display areas of increased opacity or chalky appearance, indicating subsurface damage that has disrupted the normal crystalline structure.
Surface texture changes represent another important visual indicator, with affected areas feeling rougher to tactile examination using a dental explorer. These textural modifications often correlate with underlying structural damage and may progress to frank enamel fractures if left untreated. The distribution pattern of these irregularities typically follows the direction and intensity of the traumatic force, providing valuable diagnostic information about the mechanism of injury.
Gingival tissue changes adjacent to traumatised teeth
The gingival tissues surrounding bruised teeth frequently display characteristic inflammatory responses that serve as important diagnostic indicators. These changes typically manifest as localised erythema extending from the free gingival margin to the attached gingiva, often accompanied by mild oedema that creates a slightly rounded contour compared to healthy periodontal tissues. The inflammatory response may be asymmetric, with more pronounced changes on the facial aspect of the tooth where direct trauma typically occurs.
Careful observation may reveal subtle colour variations within the gingival tissues themselves, ranging from deep red to purple hues that indicate vascular congestion and inflammatory exudate accumulation. In severe cases, small petechial haemorrhages may be visible within the attached gingiva, providing clear evidence of significant trauma to the supporting structures. These gingival changes often persist longer than initial pain symptoms, making them valuable indicators of ongoing pathological processes.
Radiographic correlation with visual findings
While visual assessment provides crucial initial diagnostic information, radiographic examination offers complementary insights into the internal structural changes accompanying tooth bruising. Periapical radiographs may reveal subtle widening of the periodontal ligament space, particularly at the apex, indicating inflammatory changes within the supporting tissues. These radiographic findings often precede visible colour changes by several days or weeks, making them valuable early diagnostic tools.
Advanced imaging techniques such as cone-beam computed tomography can reveal three-dimensional structural changes that remain invisible on conventional radiographs. These may include root fractures, alveolar bone damage, and pulp chamber modifications that significantly influence treatment planning and prognosis. The correlation between visual findings and radiographic changes provides a comprehensive picture of trauma severity and guides appropriate therapeutic interventions.
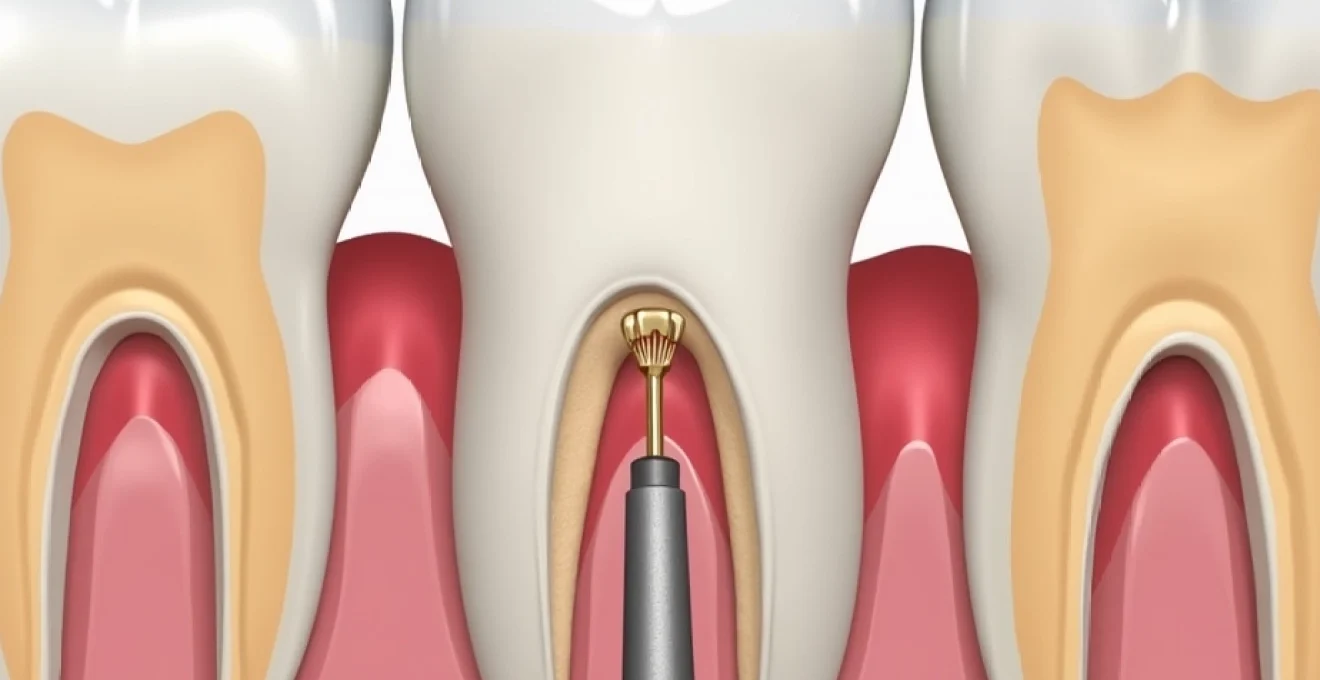
Pathophysiology of pulpal necrosis and tooth discolouration
Understanding the biological processes underlying tooth discolouration following trauma requires detailed knowledge of pulpal anatomy and the cascade of events triggered by mechanical injury. The dental pulp, contained within the rigid confines of the pulp chamber and root canals, has limited capacity to accommodate swelling and inflammatory responses. When traumatic forces damage the delicate vascular structures within the pulp, bleeding occurs in a confined space, leading to increased intrapulpal pressure and subsequent tissue ischaemia.
The progression from initial trauma to visible discolouration follows a predictable timeline influenced by factors such as patient age, tooth vitality, and the extent of vascular damage. Younger teeth with larger pulp chambers and more robust vascular supply often demonstrate greater resilience to trauma, while mature teeth with calcified pulp chambers show increased susceptibility to irreversible damage. The inflammatory response triggered by trauma involves complex interactions between immune cells, inflammatory mediators, and bacterial factors that ultimately determine whether the pulp maintains vitality or progresses to necrosis.
Haemoglobin breakdown products in dentinal tubules
The characteristic colour changes observed in bruised teeth result from the breakdown of haemoglobin and its subsequent infiltration into the dentinal tubules. Following initial bleeding within the pulp chamber, red blood cells begin to lyse, releasing haemoglobin into the surrounding tissues. This haemoglobin then undergoes oxidative breakdown, forming various chromogenic compounds that impart distinct colours to the dental tissues depending on the stage of decomposition.
The initial pink discolouration represents intact haemoglobin molecules within the dentinal tubules, while yellow-brown colours indicate the formation of biliverdin and bilirubin through normal haemoglobin catabolism. The final grey-black appearance results from the formation of iron sulphide compounds and other metallic deposits that accumulate within the dentinal matrix. These colour changes typically begin in the pulp chamber area and gradually extend coronally, creating the characteristic pattern observed in traumatised teeth.
Progressive chromogenic changes in Non-Vital teeth
The temporal progression of colour changes in non-vital teeth follows distinct phases that correlate with underlying pathological processes. The acute phase, occurring within hours to days following trauma, involves active bleeding and initial inflammatory responses that produce the characteristic pink discolouration. This stage may be reversible if appropriate treatment is instituted promptly and pulpal vitality is maintained.
The subacute phase, developing over weeks to months, involves the breakdown of cellular components and the formation of more stable chromogenic compounds. During this period, the tooth may cycle through various colour changes as different breakdown products predominate. The chronic phase, which may persist indefinitely without treatment, is characterised by the formation of stable metallic complexes and organic deposits that resist natural clearance mechanisms. Understanding these phases is crucial for determining treatment urgency and predicting long-term outcomes.
Inflammatory exudate impact on tooth transparency
Beyond colour changes, dental trauma frequently affects tooth transparency through alterations in the optical properties of enamel and dentine. Inflammatory exudate within the pulp chamber and dentinal tubules alters the refractive index of these tissues, creating areas of increased opacity that become apparent under transillumination. These changes often precede visible colour alterations and may serve as early indicators of pulpal pathology.
The loss of normal translucency typically begins in the cervical region of the crown, where the dentinal tubules are largest and most susceptible to inflammatory infiltration. As the condition progresses, the opacity extends coronally, eventually affecting the entire visible crown surface. This loss of vitality creates a characteristic “dead” appearance that experienced clinicians readily recognise, even in the absence of obvious colour changes.
Cellular debris accumulation in pulp chamber
The accumulation of cellular debris within the pulp chamber represents a significant factor in the visual changes observed following dental trauma. As pulpal tissues undergo necrosis, dead cells, inflammatory exudate, and bacterial byproducts accumulate within the confined pulp space. This debris creates a turbid environment that significantly alters the optical properties of the tooth, contributing to the characteristic loss of vitality and translucency.
The composition of this debris varies depending on the stage of pulpal breakdown and the presence of bacterial infection. Early accumulations consist primarily of inflammatory cells and plasma proteins, while later stages involve significant bacterial colonisation and the formation of putrefactive compounds. These materials not only affect tooth appearance but also contribute to the progression of periapical pathology and the development of clinical symptoms such as pain and swelling.
Differential diagnosis between bruised teeth and alternative pathologies
Accurate diagnosis of bruised teeth requires careful differentiation from other conditions that may present similar visual characteristics. Internal resorption represents one of the most challenging differential diagnoses, as it can produce pink discolouration similar to that seen in acute dental trauma. However, internal resorption typically presents with a more localised, well-defined pink area that corresponds to the resorptive defect, while traumatic bleeding tends to create more diffuse discolouration patterns.
Chronic pulpitis from carious exposure may also produce tooth discolouration, but this typically follows a different pattern and timeline compared to traumatic injury. Caries-related discolouration often begins with localised brown or black spots corresponding to areas of bacterial invasion, while trauma-induced changes typically affect the entire crown uniformly. The presence of obvious carious lesions, combined with a history of chronic pain rather than acute trauma, helps distinguish these conditions.
External cervical resorption presents another diagnostic challenge, as it may create pink discolouration in the cervical region of the tooth. However, this condition typically demonstrates a more irregular, moth-eaten appearance on radiographic examination, while traumatic injuries show more diffuse changes. The clinical history and patient symptoms also differ significantly between these conditions, with external resorption often presenting as an incidental finding rather than following acute trauma.
Understanding the subtle differences between traumatic tooth discolouration and other pathological conditions requires extensive clinical experience and systematic diagnostic approaches that combine visual assessment with comprehensive patient history and radiographic findings.
Photographic documentation techniques for dental trauma assessment
Standardised photographic documentation plays a crucial role in monitoring the progression of tooth discolouration and assessing treatment outcomes over time. Professional dental photography requires specific equipment and techniques to accurately capture subtle colour changes that may not be apparent to visual examination alone. High-resolution digital cameras equipped with macro lenses and specialised dental flash systems provide the necessary image quality for detailed documentation and analysis.
Colour accuracy represents a critical consideration in dental trauma photography, as subtle hue variations may indicate significant changes in pulpal status. Standardised lighting conditions, consistent camera settings, and appropriate colour calibration targets ensure reproducible results that enable meaningful comparisons between sequential images. The use of polarising filters can eliminate surface reflections that might obscure important visual details, particularly in the cervical regions where early colour changes typically manifest.
Digital image processing techniques can enhance the visibility of subtle colour changes that might otherwise escape detection. Histogram analysis, colour channel separation, and contrast enhancement tools enable quantitative assessment of discolouration patterns and provide objective measures of change over time. These techniques are particularly valuable for monitoring treatment response and identifying early signs of treatment failure that might require intervention modification.
The integration of standardised photography protocols into routine trauma follow-up care provides valuable documentation for both clinical decision-making and medicolegal purposes. Sequential images captured at defined intervals create a visual timeline of healing or deterioration that supports evidence-based treatment decisions. This documentation becomes particularly important in cases involving litigation or insurance claims, where objective evidence of treatment outcomes may be required.
Emergency management protocols for suspected dental contusion
The initial management of suspected dental trauma requires systematic assessment protocols that prioritise both immediate symptom relief and long-term tooth preservation. Emergency evaluation begins with comprehensive history-taking to establish the mechanism and timing of injury, followed by systematic clinical examination to identify all affected structures. Time-sensitive decision-making becomes crucial, as delays in appropriate intervention may compromise treatment outcomes and increase the likelihood of permanent complications.
Immediate pain management represents a primary concern in emergency dental trauma care, as patients often present with significant discomfort that may interfere with thorough clinical assessment. Non-steroidal anti-inflammatory drugs provide effective relief while simultaneously addressing the inflammatory component of the injury. However, careful patient screening for contraindications and appropriate dosing guidelines must be followed to ensure safe administration.
Initial pain assessment using Wong-Baker FACES scale
Standardised pain assessment tools provide objective measures of patient discomfort and enable consistent monitoring of symptom progression during treatment. The Wong-Baker FACES Scale offers particular utility in emergency dental settings, as it provides clear visual indicators that patients can easily understand and communicate. This assessment tool becomes especially valuable when treating pediatric patients or adults with communication difficulties who may struggle to articulate their pain levels accurately.
Documentation of initial pain scores provides baseline measurements for evaluating treatment effectiveness and identifying patients who may require more aggressive intervention. Serial pain assessments conducted at regular intervals help identify trends in symptom progression and may indicate developing complications such as pulpal necrosis or periapical infection. The correlation between pain scores and other clinical findings enhances diagnostic accuracy and supports evidence-based treatment decisions.
Thermal sensitivity testing with Endo-Ice application
Thermal sensitivity testing represents a fundamental component of emergency dental trauma assessment, providing valuable information about pulpal vitality and the extent of neural damage. Endo-Ice application offers a standardised method for cold testing that produces consistent results when performed according to established protocols. The technique involves brief application of frozen carbon dioxide to the facial surface of the crown, typically in the middle third, while monitoring patient response and comparing findings to adjacent unaffected teeth.
Interpretation of thermal test results requires understanding of the normal physiological responses and the modifications that occur following trauma. Healthy teeth typically respond to cold stimulation within two to three seconds with a sharp, easily localised sensation that subsides quickly upon removal of the stimulus. Traumatised teeth may demonstrate delayed responses, hypersensitivity, or complete absence of sensation, depending on the degree of neural damage present.
Electric pulp testing response evaluation
Electric pulp testing provides complementary information to thermal testing and offers particular value in cases where thermal responses may be unreliable due to recent trauma or ongoing inflammation. The technique involves application of gradually increasing electrical stimulation to the crown surface while monitoring patient response and recording threshold values. Modern electric pulp testers provide precise control over stimulation parameters and enable consistent, reproducible testing protocols.
Baseline electric pulp test values should be established for adjacent unaffected teeth to provide comparison standards and account for individual patient variations in response threshold. Traumatised teeth may demonstrate elevated thresholds, indicating neural damage, or may fail to respond entirely if complete pulpal necrosis has occurred. Serial testing over time provides valuable prognostic information and helps guide treatment planning decisions.
Percussion test methodology for periodontal ligament assessment
Percussion testing evaluates the status of periodontal ligament tissues and helps identify inflammatory changes that may not be apparent through other diagnostic methods. The test involves gentle tapping of the crown surface using a dental mirror handle or similar instrument, beginning with light pressure and gradually increasing intensity while monitoring patient response. Both vertical and lateral percussion should be performed to assess different aspects of periodontal ligament function.
Positive percussion responses indicate inflammation within the periodontal ligament space and may suggest more extensive trauma than initially apparent. The intensity and duration of percussion sensitivity often correlate with the severity of periodontal ligament damage and may predict the likelihood of developing complications such as external root resorption or ankylosis. Documentation of percussion test findings provides valuable baseline data for monitoring treatment response and identifying patients who may require more intensive follow-up care.
Systematic application of standardised diagnostic protocols in emergency dental trauma management ensures comprehensive assessment of all affected structures and supports evidence-based treatment decisions that optimise both short-term symptom relief and long-term tooth preservation.
The comprehensive evaluation of suspected dental trauma requires integration of multiple diagnostic modalities and careful interpretation of findings within the context of patient history and clinical presentation.
The integration of clinical findings, diagnostic test results, and patient-reported symptoms creates a comprehensive assessment framework that guides immediate treatment decisions and establishes appropriate monitoring protocols for optimal patient outcomes.
Emergency triage protocols must also consider the potential for multiple dental injuries that may not be immediately apparent during initial examination. Systematic evaluation of all teeth within the traumatised quadrant ensures that concurrent injuries are identified and addressed appropriately. The interconnected nature of dental structures means that forces sufficient to cause visible trauma to one tooth may have affected adjacent teeth in ways that become apparent only through comprehensive diagnostic testing.
Documentation requirements in emergency dental trauma cases extend beyond routine clinical notes to include detailed injury mechanisms, photographic evidence, and systematic recording of all diagnostic test results. This comprehensive documentation supports continuity of care during follow-up appointments and provides essential evidence for potential medicolegal proceedings. The standardisation of documentation protocols ensures that critical information is captured consistently and enables meaningful comparison of outcomes across different treatment approaches.
Patient education during emergency visits plays a crucial role in ensuring compliance with post-treatment instructions and facilitating early recognition of complications. Clear explanations of the injury mechanism, expected healing timeline, and warning signs that require immediate attention help patients become active participants in their recovery process. Effective communication strategies must account for patient anxiety and stress levels that commonly accompany dental trauma, requiring healthcare providers to balance comprehensive information delivery with emotional support and reassurance.
The success of emergency dental trauma management depends not only on accurate diagnosis and appropriate immediate treatment but also on establishing clear follow-up protocols and ensuring patient understanding of their role in the healing process.
Risk stratification protocols help identify patients who require more intensive monitoring and those who may benefit from immediate specialist referral. High-risk factors include extensive crown discolouration, multiple affected teeth, significant periodontal ligament damage, and patient factors such as immunocompromise or bleeding disorders. Early identification of these risk factors enables proactive management strategies that may prevent complications and improve long-term outcomes for traumatised teeth.
The temporal aspects of emergency dental trauma management require careful consideration of treatment timing and the biological windows for optimal intervention. Immediate stabilisation procedures may be necessary to prevent further damage, while definitive treatments such as endodontic therapy may be delayed until acute inflammation subsides. Understanding these timing considerations helps clinicians balance the need for prompt intervention with the benefits of allowing initial healing responses to occur naturally.
Follow-up appointment scheduling must account for the unpredictable nature of dental trauma healing and the potential for delayed complications to develop. Initial follow-up visits should be scheduled within 48-72 hours to assess early healing responses and modify treatment plans as necessary. Subsequent appointments at regular intervals enable monitoring of colour changes, pulpal vitality, and the development of any complications that may require additional intervention. The frequency and duration of follow-up care depend on injury severity, patient risk factors, and initial treatment response patterns observed during early healing phases.